
Robotic training devices have firmly claimed their place in modern rehabilitation. From mobile exoskeletons to therapeutic assistive systems, rehabilitation centers are increasingly using technology to improve patients’ walking ability. While many of these devices show promise for gait rehabilitation, their rapid introduction into clinical practice also raises questions. How can we best employ these devices in practice? Which patients are most likely to benefit? And which functional goals are they able to support?
Almost five years ago, a new robotic harnessing system (RYSEN from Motek Medical) was introduced at Heliomare Rehabilitation Center (Wijk aan Zee, the Netherlands). This body weight support system assists patients during standing and walking by partially unloading the body, enabling early and safe gait training. The device allows patients to walk freely in all directions while receiving adjustable body weight support. What makes a system like the RYSEN unique is that support is not limited to vertical unloading. It can also provide forward, backward, and sideward forces (scan QR in Figure 1 for videos). This opens up possibilities to challenge balance, stimulate propulsion, or assist stability. On top of that, the system integrates augmented reality, projecting interactive games onto the floor, which may facilitate motor learning. Notably, the RYSEN is one example within a growing class of multidirectional, overground body weight support systems, with comparable devices such as the FLOAT by RehaStim also available.
With so many possible avenues for intervention, therapists started asking questions: What training goals can we target? How much support should we give? How do we choose the right force settings?
These questions formed the basis of my PhD project. In observational studies, we explored which percentages of body weight support were chosen and what goals were pursued in current clinical practice. In experimental studies, we investigated the effects of vertical, forward, backward, and sideward forces on gait parameters and muscle activity to find out if they could evoke desired adaptations in gait in people after stroke and spinal cord injury (e.g. see Figure 1).
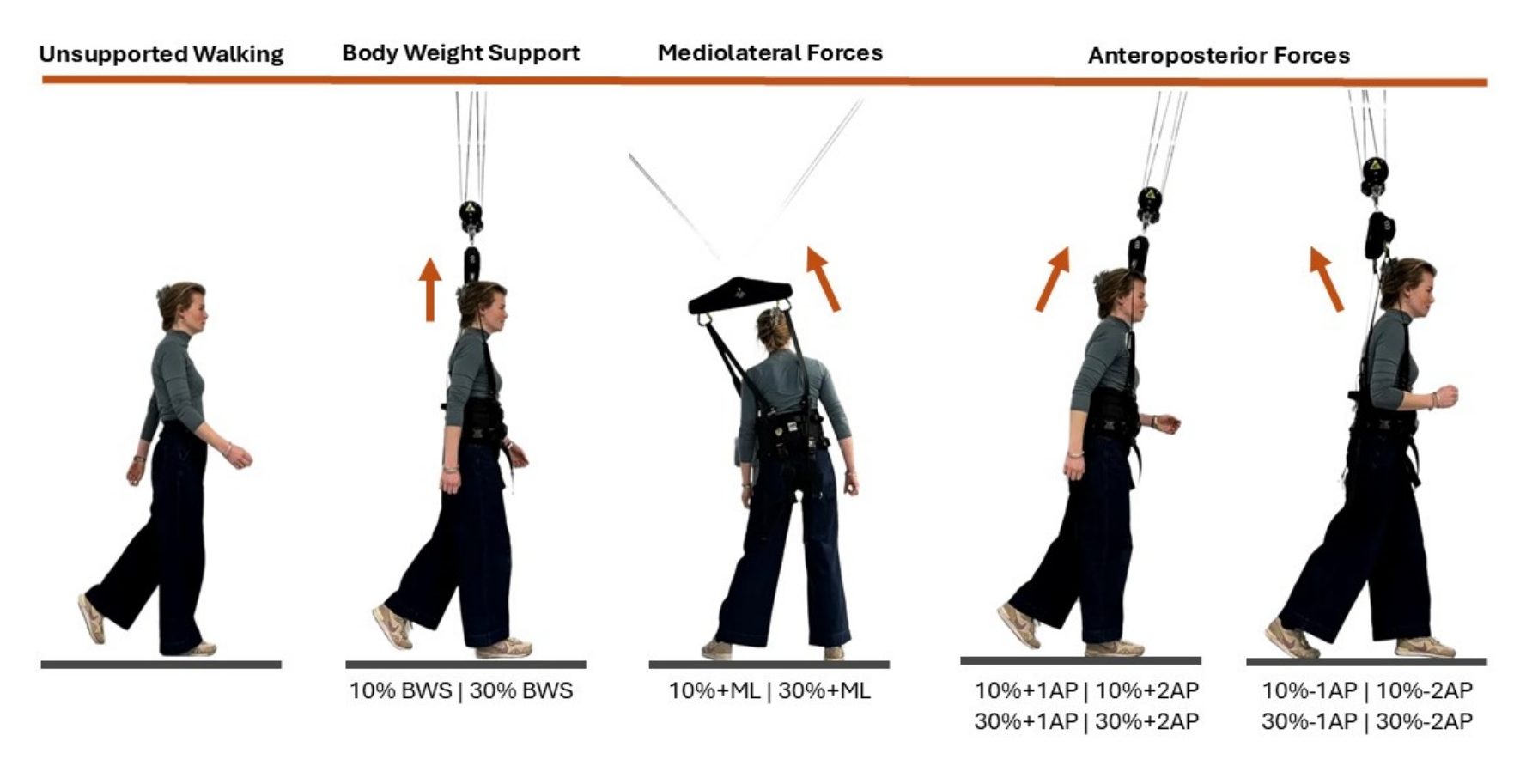

Figure 1. Schematic overview of the different experimental RYSEN conditions. Scan the QR code to view videos. BWS: body weight support; ML: mediolateral forces; AP: anteroposterior forces.
The emerging findings are encouraging. Our observational study demonstrated that the RYSEN is well accepted by both patients and therapists, and that augmented reality–based games enhanced participants’ confidence in balance during training. However, differences in training goals and intensity between modalities were limited, suggesting that further research and implementation strategies are needed to fully realize the device’s potential. Experimental studies indicated promising opportunities for targeted gait training. For example, in individuals with incomplete spinal cord injury, even small amounts of vertical body weight support (10%) resulted in an approximately 10% improvement in balance confidence. Additionally, the application of mediolateral forces, restricting sideward movement with a contrary-directed force, produced changes in step parameters and muscle activity consistent with enhanced balance control, including a narrower step width and reduced activity of the tibialis anterior and peroneus longus muscles, which are primary involved in the mediolateral ankle balance strategy (Figure 2).
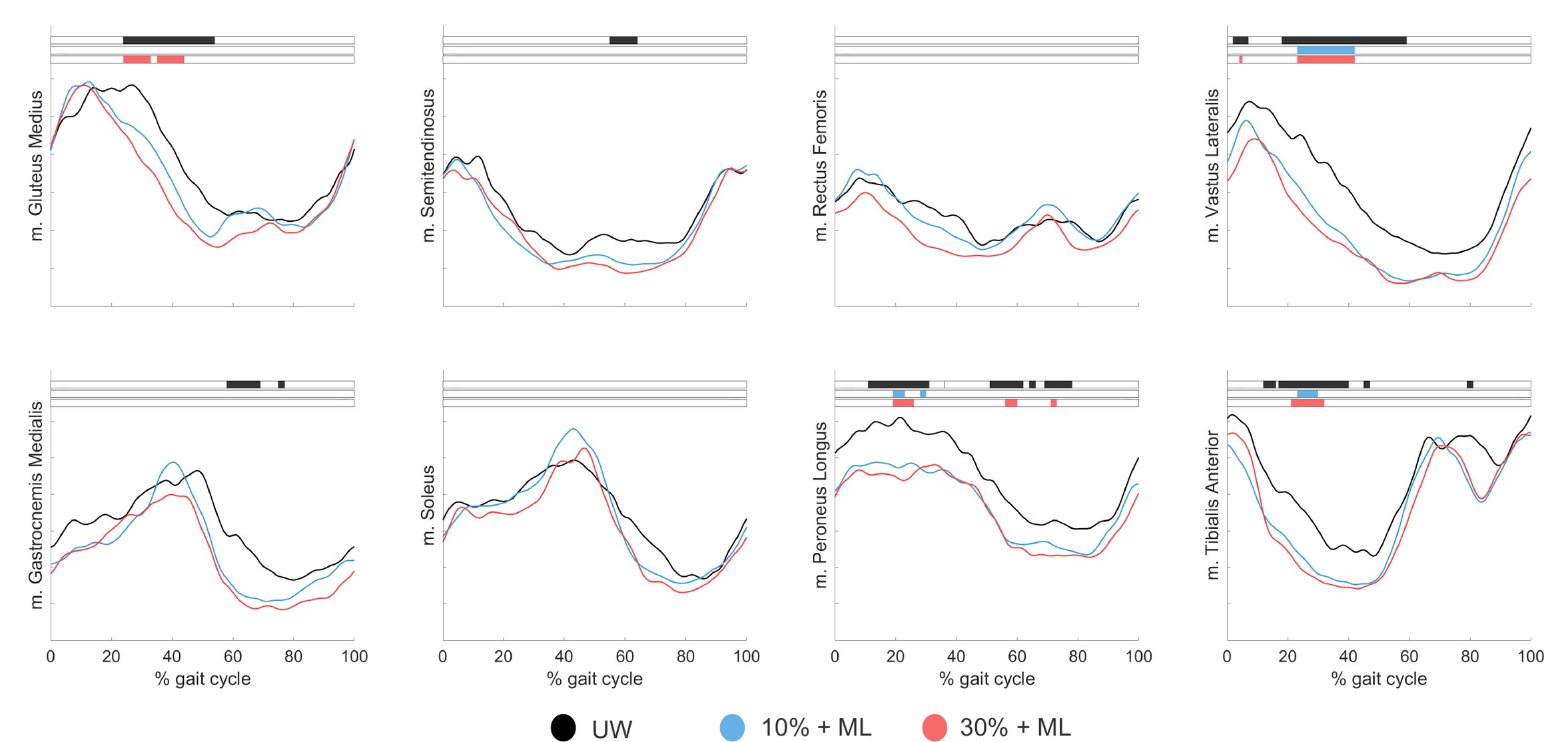
Figure 2. Mean muscle activation patterns across the gait cycle during with mediolateral (ML) forces for individuals with incomplete spinal cord injury (n=15) during Unsupported Walking (UW; black), 10 % BWS + mediolateral forces (blue) and 30 % BWS + mediolateral forces (red). The colored lines represent mean values for the different conditions. Horizontal boxes at the top of each figure represent the part of the gait cycle where significant differences occur, based on statistical parametric mapping (SPM). The main effect is shown in black and post-hoc effects are shown in blue and pink.
Our results provide valuable first insights into the potential effects of multidirectional body weight support, but guidelines for structured application in clinical practice are still limited. Fully unlocking the potential and clinical application of robotic harnessing devices like the RYSEN (and similar devices such as RehaStim’s FLOAT) therefore requires continued collaboration between researchers, engineers, clinicians, and patients. Future studies could explore the use of explicit training instructions and the integration of therapeutic exercises to determine if and how effects on motor control (and ultimately: functioning) can be optimized across different clinical populations and settings.
On January 19, 2026, I defended my thesis at the University of Groningen, the Netherlands. The project was supervised by prof. dr. Han Houdijk, prof. dr. Coen van Bennekom, dr. Tom Buurke, and dr. Sina David. For those interested in the details, the full thesis can be found here.
About the Author

Dr. Sanne Ettema is a postdoctoral researcher at the Department of Rehabilitation of the Amsterdam University Medical Center, the Netherlands. Her main research interests are the control of balance and walking in clinical populations, with a focus on motor control, biomechanics, and application in clinical practice.
Copyright
© 2021 by the author. Except as otherwise noted, the ISPGR blog, including its text and figures, is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/4.0/legalcode.
ISPGR blog (ISSN 2561-4703)
Are you interested in writing a blog post for the ISPGR website? If so, please email the ISGPR Secretariat with the following information:
- First and Last Name
- Institution/Affiliation
- Paper you will be referencing

