
Following a stroke, it is important to assess a person’s perception of verticality. This assessment can help us to find what causes the bodily disorientation with respect to vertical (lateropulsion) and can guide post-stroke rehabilitation and monitor postural recovery. The visual vertical (VV) is the most commonly used test to assess verticality perception, both in research and in clinical practice. It is a simple test that consists of adjusting a luminous rod to the vertical in darkness; however, specific guidelines for use in clinical practice are lacking. Published studies have used different methodologies and the impact of these different methodologies on the assessment outcome is not well-understood. For example, should the trunk and head be free to move during the test or should they be fixed in the upright position? This question is critical for stroke survivors. It is well-known that spontaneous lateral whole body tilts are common after stroke and this may compromise their ability to sit on their own and might further impact their perception of verticality. In the present study, we aimed to analyse the impact of controlling body orientation on stroke patients’ ability to estimate VV and their ability to sit unsupported.
VV perception was assessed in 20 controls and 36 subacute patients undergoing rehabilitation after a first hemisphere stroke, under 3 different scenarios: body not fixed (trunk and head free), partially fixed (trunk fixed, head free), or both trunk and head were fixed. We quantified both trunk and head orientations and analysed VV as a function of trunk and head tilt. Patients were classified into 2 groups according to their ability to maintain (n=25) or not (n=11) an independent upright sitting posture. Our results confirmed for the first time the clinical intuition: it is spontaneous upright trunk (and not head) orientation which is necessary for recovering an independent sitting posture after stroke. This suggests that postural orientation deficits, especially trunk orientation, are a major cause of lateral postural disorders after a stroke. The level of fixation strongly affects the estimation of VV in stroke patients who have difficulties maintaining a seated posture. Our results suggest that a fixed trunk and head in the upright position was the most optimal setting for assessing VV. We proposed that measuring VV without any body fixation is only valid in patients with satisfactory balance abilities. Our results contribute to a better standardization of VV assessment to optimize its integration in research and clinical practice.
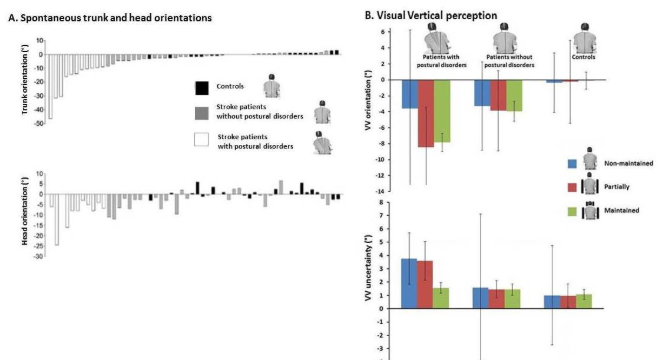
Figure. Individual mean spontaneous orientations of trunk axis and head axis. The data were classified from the most pronounced contralesional tilt (negative values) to the most pronounced ipsilesional tilt (positive values), for trunk orientation, and this order was maintained for the classification of head orientation data. (B) Visual vertical perception, orientation (mean) and uncertainty (variability) as a function of group and setting.
Publications
Piscicelli C, Barra J, Sibille B, Bourdillon C, Guerraz M, Pérennou D. (2016). Maintaining trunk and head upright optimizes visual vertical measurement after stroke, Neurorehabil Neural Repair, 30(1):9-18. https://doi.org/10.1177/1545968315583722
Piscicelli C, Pérennou D. (2017). Visual verticality perception after stroke: A systematic review of methodological approaches and suggestions for standardization. Ann Phys Rehabil Med, 11. pii: S1877-0657(16)00042-7. https://doi.org/10.1016/j.rehab.2016.02.004
About the Author

Céline Piscicelli and Dominic Pérennou
University Hospital Grenoble-Alpes
Celine Piscicelli received her PhD in Cognitive Psychology and Neuroscience from Grenoble-Alpes University. She currently works as a neuropsychologist in the Physical and Rehabilitation Medicine Unit at University Hospital Grenoble-Alpes and is an associate member in the Psychology and Neurocognition Lab at Grenoble-Alpes University. Her research focuses on spatial cognition and its interaction with posture and action.
Dominic Pérennou is Professor of Medicine, Chair of Physical Medicine and Rehabilitation at Grenoble-Alpes University, and head of the Department of Neurorehabilitation at the University Hospital Grenoble-Alpes (France). He is Editor in Chief of the Annals of Physical Medicine and Rehabilitation, and Associate Editor of Gait & Posture. His main research focuses on internals models of verticality for postural and gait control.
Copyright
© 2018 by the author. Except as otherwise noted, the ISPGR blog, including its text and figures, is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by-sa/4.0/legalcode.
ISPGR blog (ISSN 2561-4703)
Are you interested in writing a blog post for the ISPGR website? If so, please email the ISGPR Secretariat with the following information:
- First and Last Name
- Institution/Affiliation
- Paper you will be referencing